
Why Sustainable Transportation Advocates Need to Talk About Abortion Access

America’s auto-centric transportation system already poses a massive barrier to abortion care for people without the resources to travel long distances by car — and the likely rollback of the decision that guarantees U.S. residents the right to key reproductive rights could make that hurdle virtually insurmountable for countless U.S. residents, advocates say.
If the Supreme Court indeed overturns its Roe v. Wade precedent, experts say it will drastically increase the challenges of obtaining pregnancy-terminating procedures at safe and legal clinics — not the least of which is the travel required to reach them in the first place.
“Increases in driving distances would pose hurdles for many people,” Dr. Herminia Palacio, president and CEO of the Guttmacher Institute, said in a release. “However, research shows that some groups of people are disproportionately affected by abortion restrictions — including those with low incomes, people of color, young people, LGBTQ individuals and people in many rural communities.”
The Guttmacher Institute recently quantified how far U.S. residents would have to travel if the justices do, indeed, overturn Roe:
Of course, some of those vulnerable groups — people of color, low-income people and the young — are also among the groups least likely to drive at all. And that could put them in an even more vulnerable position if state reproductive choice laws shift as expected.
Currently, 22 states have laws on the books that would immediately trigger a total abortion ban should Roe v. Wade (and its companion decision, Planned Parenthood v. Casey) be reversed, and four more are considered highly likely to adopt bans of their own. Those states include some of America’s largest by total land mass, and many are also located in sprawling, transit-poor regions where many neighboring states are also expected to enact abortion bans — a phenomenon experts refer to as “abortion deserts.”
For residents of those communities, that means the average distance to the specialized clinics where 95 percent of documented pregnancy terminations are now performed would multiply to unprecedented levels, functionally rendering care inaccessible to untold numbers of women, transgender men, and non-binary people.
Those states include:
- Louisiana, where the average one-way travel distance to the nearest provider would swell to 630 miles or a 1,720-percent increase over current averages.
- Florida (567 miles, a 6,803-percent increase)
- Texas (525 miles, a 3,017-percent increase)
- Mississippi (428 miles, a 638-percent increase)
- Utah (247 miles, a 837-percent increase)
Even those stunning averages, though, don’t fully capture the burden of being forced to travel long distances in order to access basic reproductive care — particularly for pregnant people who don’t have reliable access to personal vehicles.
A 2017 Guttmacher survey of patients who had to cross state lines or travel more than 100 miles to terminate a pregnancy found that “the distance itself was not what made traveling burdensome; external factors (e.g., inclement weather, limited access to safe and reliable transportation, or the need to use multiple means of transport) significantly increased the time it took women to travel even relatively short distances to care.”
Put another way: even the 22 miles it takes the average abortion seeker has to travel can be profoundly punishing if she has to, say, catch three unreliable buses and walk part of the way in the rain.
And that’s before all the other barriers to care are factored in, like appointment availability at overburdened clinics forced to absorb an influx of patients from abortion deserts, the cost of the procedure, follow-up care, and any associated travel and accommodations, the ability to get time off work or secure childcare, racist and transphobic doctors, and so much more.
Those barriers, collectively, bump the average one-way distance a U.S. resident actually travels to terminate a pregnancy up to 36 miles each way — because about half of abortion patients don’t, or can’t, utilize their closest available clinic.
Let’s be clear: ending car dependence alone will not put real reproductive choice within reach of every U.S. resident — nor will it necessarily put any other kind of critical care within reach, either.
Access to quality, affordable, convenient, and safe medical treatment is not simply a matter of being able to physically access a doctor. Restructuring America’s broken healthcare system is among the most critical, urgent, and daunting challenges of modern times.
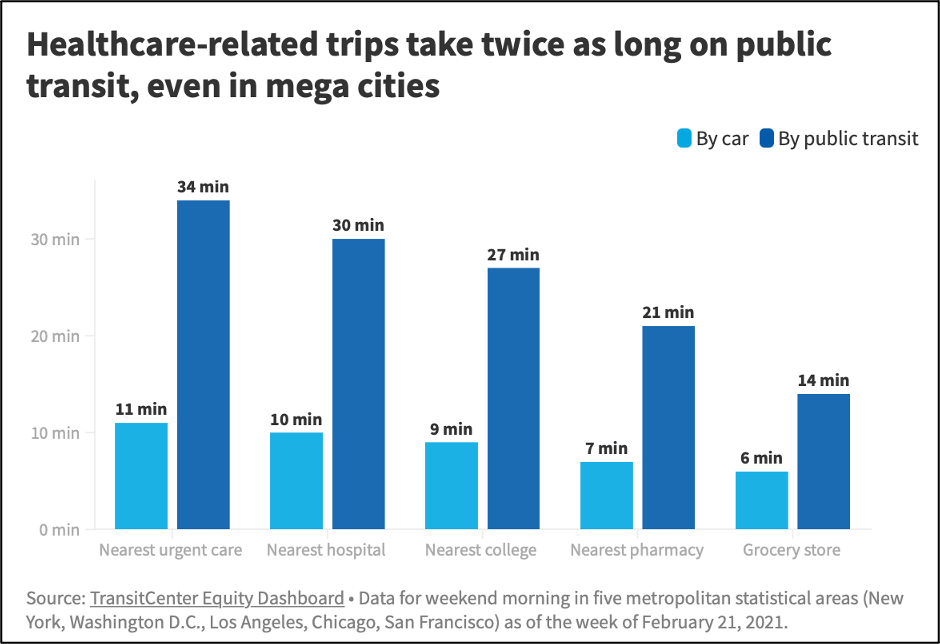
But as long as we continue to center our transportation and land use choices around the private automobile, our built environment will continue to compound the challenges of accessing medical treatment. It will still take more than three times as long to access an urgent care facility on public transit than it does in a private vehicle. Residents will still delay care, miss appointments, and skip necessary medications simply because they cannot get where they need to go.
When it comes to reproductive choices, it will not mean that fewer people will get abortions. But it will mean more people will die from lack of access to safe and legal abortion providers in their home communities — and over time, from all the long, dangerous, and polluting drives U.S. residents will be forced into take in order to reach the care they need somewhere else.

Streetsblog has migrated to a new comment system. New commenters can register directly in the comments section of any article. Returning commenters: your previous comments and display name have been preserved, but you'll need to reclaim your account by clicking "Forgot your password?" on the sign-in form, entering your email, and following the verification link to set a new password — this is required because passwords could not be carried over during the migration. For questions, contact tips@streetsblog.org.




